Published on LinkedIn: https://www.linkedin.com/pulse/when-ok-cheat-win-business-oliver-canty
An independent test of the same parameters by Butterworth gave similar results:
Surface deposits after single cycle:
Silver nitrate is persistent in the environment, and will build up cumulatively each time a room is processed. The permitted level of silver nitrate dust in the air is vanishingly small. The legal maximum is 0.01mg/m³ – 250 times this amount of the chemical is deposited on each square metre of surface per process!
This presents a particular danger to hospital staff making up the bed after a Deprox process – laying down the mattress and placing sheets will disturb clouds of the fine dust at very hazardous levels. Staff should certainly be provided with appropriate respiratory equipment for this task, and silver nitrate dust levels should be monitored before readmitting patients.
Rooms that have become heavily contaminated by multiple processes may need decontaminating by Hazchem professionals.

Isolation rooms at the Royal Liverpool University Hospital have become so heavily contaminated with silver nitrate that patients have complained, mistaking the black deposits on the windows for dirt. Director of nursing Lisa Grant admitted that the Hydrogen Peroxide Vapour (HPV) bio-decontamination system leaves a “sterile residue” but was apparently unaware that it is silver nitrate. The photo above was submitted to The Liverpool Echo by a patient who attempted to remove the chemical with a tissue. There is enough silver nitrate on the tissue to cause unpleasant chemical burns to the skin. Even more seriously, the AgNO3 dust levels in the room must have been far in excess of the legal maximum, which is an invisibly small 0.01mg/m³ – that’s 1/100,000th of a gram per cubic metre of air.
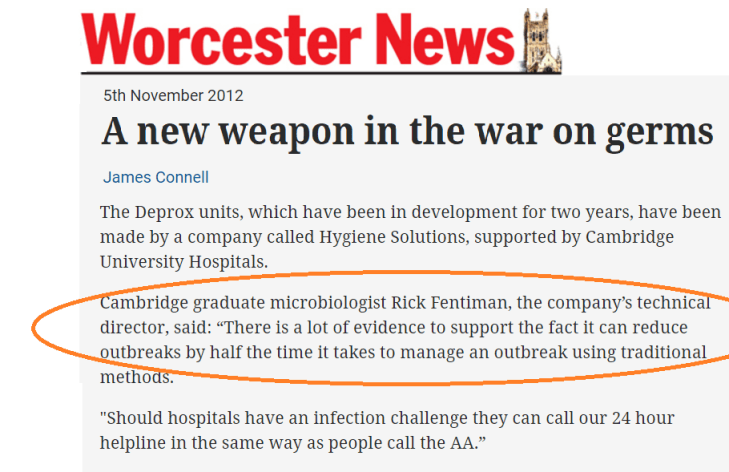
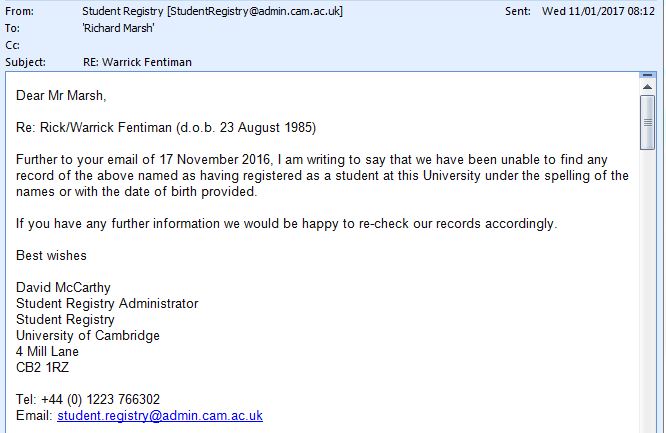
A letter published this week by Prof. Wilson of UCLH finally proves how Hygiene Solutions’ (Deprox) director Rick Fentiman cheated both the UCLH and rival HPV system manufacturer Bioquell Plc, in a widely publicized comparative test in 2015. The results of this test apparently demonstrated that the Deprox, vapourising a 5% Hydrogen peroxide solution had identical germicidal efficacy as the Bioquell system vapourising 35% hydrogen peroxide solution.
I published an article in 2016 in which I analyzed the test results as published by Professor Wilson and colleagues in the Journal of Hospital Infection, and concluded that Fentiman had in fact filled the internal tank of the Deprox machine with a 35% solution prior to the test. New data published in the letter proves this claim beyond reasonable doubt.
In Wilson’s original test, neither the aerial concentration of H2O2 vapour , or the concentration of the liquid solutions was measured.
In response to widespread concern and comment as to the rather surprising results obtained, Wilson recently again obtained the use of a Bioquell and a Deprox system and measured the concentrations of both the liquid and aerial vapour phases throughout their test cycles, as detailed in this week’s letter.
The Deprox was using 5% H2O2 solution, and produced peak vapour concentrations of 29 to 46ppm. The Bioquell machine was using a 35% solution, and produced 450 to 640ppm of vapour.
The maximum aerial concentration of H2O2 that can be generated is limited by the concentration of the original solution. Henry’s law can be used to prove that about 50ppm is the maximum sustained aerial concentration that can be generated from a 5% solution. The figure of 46ppm for Deprox from Wilson’s retest of the machine is thus exactly what would be expected.
In the original comparative test, both the Deprox and the Bioquell systems demonstrated practically identical efficacies of log 5.1 for spores and log 6.3 for vegetative bacteria. A very large number of biological indicators of several species were used over multiple tests, and no significant difference in performance between the two systems was found.
Therefore, inescapably, both systems must have generated the same aerial concentration of H2O2 vapour, and that must have been in the region of 400 to 700ppm. (There are numerous published papers demonstrating a log 6 efficacy for HPV systems using 30-35% H2O2 solutions)
It is physically impossible to generate anything close to these levels of vapour by evaporating or aerosolizing a 5% solution. Quite apart from Henry’s law, the volume of water that would have to be evaporated along with the H2O2 would quickly push the relative humidity to saturation, and prevent further evaporation from taking place.
How then was this deception accomplished?
There are some aspects of the way in which the original UCLH tests were conducted that are very suggestive:
At the time of the tests, Hygiene Solutions had a contract with UCLH, and had 4 Deprox machines permanently on site, which were operated daily by Hygiene Solutions employees. UCLH had a definite rule that the equipment was not to be operated by their staff – hence no UCLH staff were trained in the use of the equipment.
The paper states: “The HPS1 unit was operated by a trained engineer (Bioquell), while the HPS2 module was operated by hospital staff following training by a dedicated member of the issuing manufacturer (i.e. Hygiene Solutions).”
I have two independent witnesses that the two Deprox machines were used in the trial were not the machines already on site, but were specially prepared at the Kings Lynn depot, with all new piezo discs and calatytic deactivation media. The machines were driven up to UCLH personally by Rick Fentiman, who stayed for the duration of the tests then drove the machines back to Lynn. Apparently no other Hygiene Solutions staff were involved. The “dedicated member” therefore was Rick Fentiman, and he instructed and supervised some unidentified member of the “hospital staff” in the operation of the equipment “on the spot”.
The paper says: “However, during this study, both parties provided storage of equipment and hydrogen peroxide stock solutions off-site.” In the case of the Deprox units, this was the large van in which they were transported. Clearly then there would have been opportunity for Mr Fentiman to have filled the internal storage tank of the test machines with a 35% solution and disposed of or diluted any residual fluid after the test, without either his own employees or the UCLH staff being aware of the substitution.
It is pertinent that (unknown to the UCLH) the Deprox has a substantial internal storage tank, of about 8 litres capacity.

Illustration from the Deprox patent.
The evaporation unit draws from the bottom of this tank, and the 2 litre Deproxin refill bottles trickle feed in to the top of the tank. I assume that for the sake of authenticity, a genuine Deproxin refill was inserted in to the top of the machine for the tests, hence even if Prof Wilson had tested the concentration of the fluid, he would have found it to be as stated. As concentrated H2O2 solution is substantially denser than water, a trickle of dilute solution in to the top of the tank would have no significant effect over the course of a few cycles of the machine.

Deprox salesman Tom Lister stalls when faced with a direct question about the UCLH tests. The machines had been filled with a 35% hydrogen peroxide solution, where UCLH were told it was a 5% solution. Tom knows this, and his guilty conscience shows very clearly in his body language and facial expressions. Rather than answer he says “Where did you say you were from?” although I had just told him, and was wearing a badge with the answer in large type!
In a letter published today in the Journal of Hospital Infection, Professor Peter Wilson and colleagues report on their retesting of the Deprox (Hygiene Solutions Ltd) HPV decontamination system. The retesting was in response to concerns widely raised that the earlier tests of the system, which purported to give a log 6 efficacy, were the result of the manufacturer misrepresenting the concentration and/or constituents of the Deproxin solution.
In brief, the retest reveals the following:
It is very much to the credit of Professor Wilson and colleagues that they have thoroughly retested the system in response to widespread concerns. It is sad that commercial interests would abuse the trust and confidence of highly qualified academics in this way by misrepresenting the basic test parameters.
For those without access to the Journal of Hospital Infection, I have reproduced the letter below, and a PDF is downloadable here.
Sir,
In response to the letter from Dr Singh commenting on our paper.[1], [2]
The objective of our study was to evaluate the reductions in environmental contamination during in-use operation of two commercially-available hydrogen peroxide whole-room disinfection systems.2 Both manufacturers agreed test parameters prior to the trial to ensure methodology followed manufacturer instructions. Our findings suggested similar efficacy of the two systems against both surface contamination and biological indicators of common pathogens. Inocula used on the indicators far exceeded the likely levels seen in the environment.
Additional studies were performed as part of the original work using the same methodology with four strains each of MRSA, Klebsiella pneumoniae, Clostridium difficile spores and Acinetobacter baumannii. Three HPV decontamination cycles were evaluated for each system. Of 305/320 samples, >4-log10 reduction was achieved.
Aerial concentrations of hydrogen peroxide and relative humidity were monitored continuously during a further 6 cycles of both systems using a sensor (C-16 Portasens II Gas Detector; Analytical Technology Inc., Collegeville, PA, USA). In addition, horizontal surfaces in the near-patient vicinity were swabbed and analysed to detect fallout of silver and nitrate at the end of HPV decontamination cycles (n=3). Surfaces were swabbed and analysed for silver by titration (Silver Test Kit, DTK Water, Wellingborough, UK) and nitrate using Quantofix semi-quantitative test strips (Macherey-Nagel, Düren, Germany).
For the Deprox (Hygiene Solutions, King’s Lynn, UK) system, peak aerial values of 29-46 ppm hydrogen peroxide were achieved with similar bacteriological efficacy as other cycles. The mean level at the end of the cycles was 3.3ppm for 41.8% (30.8-58.1%) mean relative humidity at start of cycles. Silver and nitrate were detected on surfaces at 1.5-2.5mg/m2 following cycles with the Deprox system.
For the Bioquell Q10 system with the R10 aeration unit (Bioquell, Andover, UK), the peak aerial levels of hydrogen peroxide were 450-640ppm. The mean level at the end of the cycles was 0.0ppm with starting mean relative humidity 42.5% (34.5-49.7%). No silver or nitrate was detected on surfaces following cycles with the Bioquell Q10 system.
The aqueous concentration of hydrogen peroxide in a Hygiene Solutions cartridge (Deprox) tested on one occasion at the point of insertion into the machine was 5%. Nitrate was detected in the aqueous solution at 10-25mg/L. The aqueous hydrogen peroxide concentration in the Bioquell Q10 cartridge (Bioquell HPV-AQ) was 35% and no silver or nitrate was detected.
Dr Singh suggests C. difficile spores (but not the other organisms) persisted underneath the bed and on the window frame after decontamination using the Deprox system. The persistence of spores may have been minimised during the Bioquell Q10 cycles by the inclusion of an oscillating fan to facilitate aerial distribution and aid breakdown of hydrogen peroxide vapour.
As Dr Singh suggests, settling of active silver onto biological indicator coupons during a cycle of aerial HPV decontamination may have contributed to the bactericidal/sporicidal activity of the Deprox system. However further studies would be required to elucidate its role.

At the Regina Court this morning, F. William Johnson, QC., BA., LL.B., B.C.L. (OXON) representing Specialist Hygiene Solutions Ltd, preempted the proceedings by requesting an adjournment as instructed by his client.
I have no doubt whatever that the unprecedented response to yesterday’s deproxfraud.info post is the reason for this abrupt about-turn.
By the end of the day, that one article had received a staggering 595 hits, and this in spite of the USA being otherwise occupied. The top 5 countries of origin are listed below:

A heartfelt thank you to everyone who visited the site, and especially to those who spread the word via social media to achieve this resounding endorsement of the battle against corrupt medical equipment manufacturers.
Since the news of Fentiman’s intended legal action was published, late on July 3rd, the blog posts have received an unprecedented 1349 views, 373 of which were from Australia and New Zealand. At the time of writing, 10.22am July 6th, today’s views are already at 190 and rising fast!
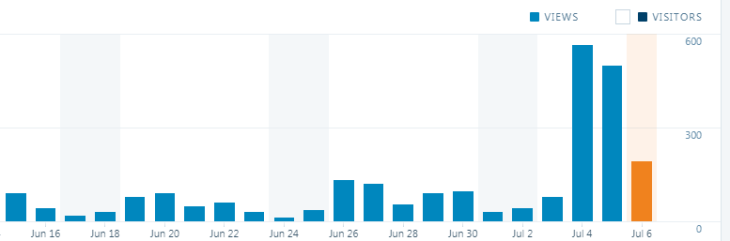
deproxfraud.info views as of 10.22 am July 6th.

Regina Courthouse
On Wednesday 5th July 2017, Hygiene Solutions Ltd. will attempt to register a gagging order against Richard Marsh, a former Deprox engineer, in an attempt to close down the highly embarrassing deproxfraud.info website.
The hearing will be before The Honourable Mr. Justice B.A. Barrington-Foote, who had already rejected a previous submission from Fentiman on the same lines. The case is at 9.00am, at the Regina Court of the Queen’s Bench, 2425 Victoria Avenue, Regina, SK S4P 4W6, Phone: (306) 787-5377.
The hearing is open to the public, and the documents filed in connection with the case may be examined and copied at the Registrar’s desk in the Courthouse.
It is of note that after 9 months and (as of this afternoon) 35,634 views of deproxfraud.info, Hygiene Solutions has finally attempted this legal action by way of an obscure legal instrument called a “Tomlin Order”. If the shocking allegations made by deproxfraud.info are false, as Fentiman and Co. maintain, why wouldn’t they have sued for libel and defamation in September when the website was first published?
While the application is expected to fail, deproxfraud.info will continue publication regardless of the outcome.
This post has broken the record for daily hits. Since publication yesterday afternoon, this post has received 553 hits and still rising fast. The daily total is expected to top 600.


Judge Adele Williams
Judgement was pronounced on a £26,000 NHS fraud last week. The perpetrators only escaped jail as they had pleaded guilty at the earliest opportunity and had repaid the money in full.
But Judge Adele Williams described it as a
She said further: –
What would the Judge have to say to the perpetrators of an £8,000,000 fraud against the NHS? Even if the directors of Hygiene Solutions were to refund the NHS for the tens of thousands of fraudulent Deprox processes they have done over the years, (see https://deproxfraud.info/2017/03/13/leaked-emails-prove-test-cheating-bodily-harm-and-massive-fraud/ ) would they escape jail?

Spare a thought for the unfortunate patients of Yeovil Hospital wards 7B and 8B. With the two wards hit by a nasty Norovirus outbreak, Director of Nursing Shelagh Meldrum is proposing to eliminate the germs WITHOUT the use of bleach or other “harmful chemicals” (i.e. disinfectant). Instead, she will put her trust (and her patient’s lives) into the hands of the notorious fake medical equipment company, Hygiene Solutions Ltd of King’s Lynn.
The Ultra-V sounds like something from science fiction. Unfortunately, that is exactly what it is. A cheaply reverse-engineered copy of an obsolete American device, built in the back of a farm sundries warehouse, the Ultra-V is foisted on unsuspecting NHS by unctuous salesmen armed with a pack of outrageous lies, which can be disproved by anyone with a basic understanding of physics.
UV-C light, as generated by the Ultra-V is well known for its germicidal properties. So what exactly is the problem with the Ultra-V, and why should the hospital not use this instead of bleach?
The problem is that light travels in straight lines, and hence casts shadows. This is very evident from the photo of a crescent moon above. The dark side is very dark indeed, the sunlight does NOT wrap around corners to light up the lunar night. This is just as true for UV light as for any other wavelength. Otherwise you could get a suntan at night.
Shadowed areas in a hospital room are not exposed to the UV radiation, hence are not disinfected. Conventional UV-C systems deal with the problem by using two or three light emitting units placed around the room to eliminate the shadowed areas, or otherwise require the unit to perform two disinfection cycles from two different locations in the room, thus ensuring that all areas are exposed at least once.
According to their sales brochure, the Ultra-V, by some miracle of optical technology can reach “shadowed areas, under bedside units and hidden corners” all from “one central location within each room”.
This miracle is achieved by “Spectromes”. These are apparently small light meters that are placed around the room to ensure that all surfaces get fully exposed. The exposure time is theoretically extended until the darkest “Spectrome” has had a full dose.
The only UV light received by a Spectrome that is in a shadow is the diffuse reflections from the lit surfaces of the room. Unfortunately most substances absorb UV-C radiation very strongly – far more than they do for visible light. In the UV-C world, almost everything non-metallic looks black.
Typical hospital surfaces absorb 95% of UV-C radiation, and scatter the rest. It follows that the shadowed areas are very dark, as at the most they can expect to receive 1/20th of the radiation of the directly lit areas. Consequently, if this scattered light is to disinfect the shadows, the process will have to be extended in duration 20 fold. Is this what happens?
No.
The normal process time with the Spectromes fully exposed is 15 to 20 minutes. Place a Spectrome in the shadows, and the process might extend to 40 minutes at the max. (Try it, if you don’t believe me.) At this point, the Ultra-V is programmed to override the Spectrome, and turn out the UV lights, indicating that the process is complete. Just in case hospital staff might be suspicious, the Ultra-V automatically sends a cheerful email to the operator’s designated address, giving time, date location, and certifying that the room has been decontaminated to a log 4 to 6 standard.
To give an example of how dangerous this is, consider the bedrails on a standard hospital bed – these are high touch areas constantly exposed to the patient’s hands and every cough and sneeze. From its “single central location” the Ultra-V unit, obviously and indisputably will only illuminate one side of each bed rail. The other side will be nearly as dark, in UV terms, as the dark side of the moon in the photo above. A standard Ultra-V process will leave these areas highly contaminated. A simple test with standard Biological Indicator coupons will prove this. (Again, don’t take my word for it – try it.)
To compound the error, the Spectromes are narrow bottomed plastic boxes that have to be placed on a hard, level surface, usually the floor or a bedside cabinet. it is completely impossible for them to monitor small, high touch areas like the back of a bedrail.

So on the positive side, at least the unshadowed areas will get a thorough log 4 to log 6 clean? Sadly not. The following Journal of Hospital Infection article detailing a study at the Wye Valley NHS Trust, demonstrated an efficacy of less than log 1 for the Ultra-V.
The outlook for the patients of Yeovil hospital does not look very bright, at any wavelength, unless there is a change of heart.
Please Shelagh Meldrum, for the sake of both patients and staff, don’t throw away the bleach just yet…use your £50,000 white elephant if you must, but give the wards a good old-fashioned hypochlorite deep clean first!

Move over Wikileaks – now we have Ricki-leaks…
A large batch of very interesting internal Hygiene Solutions emails have fortuitously come into my possession. Too much material for one post so this will just be the first of three…
In January 2015, Mark Fentiman sent an urgent message that all Deprox units were to be turned down to RH5. Now it emerges that this order was in response to the incident above, in which a healthcare worker at the Royal Worcester Hospital inhaled Deproxin fumes and suffered serious respiratory problems. (Note that ISS Healthcare operate the Deprox machines as a subcontractor in some NHS hospitals.)
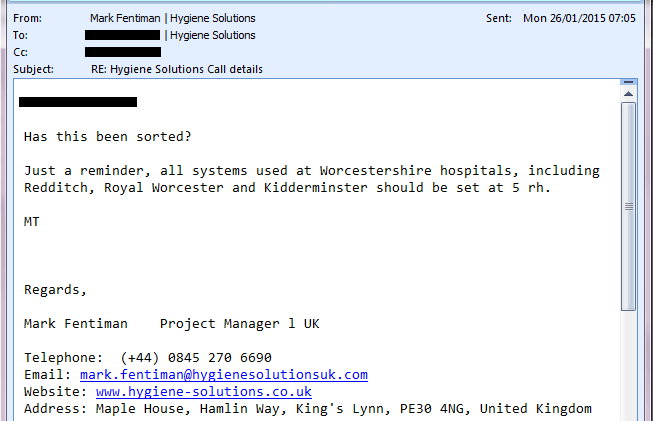
The Log6 claim so loudly and insistently trumpeted by Hygiene Solutions is based on a machine set to RH40. The RH setting gives the amount of H2O2 per cubic metre of air, so resetting the machine to RH5 only gives 12% of the required concentration. In reality, the machine is just a placebo – no useful or meaningful level of disinfection is possible at this level.
The shocking fact is that Hygiene Solutions continued to provide their Deprox systems and “decontamination” service at this dangerous and utterly ineffective level, did not inform their 60 or so NHS Hospital customers of the change, and continued to charge full price, a tidy sum of £2,500,000 per year.
Given that approximately 5000 NHS patients die each year from the very infections that this system is supposed to prevent, there can be no doubt that this action led to completely avoidable infections and death, as well as robbing the NHS of millions of pounds in fees for thousands of imaginary decontamination services that did not actually take place.
To follow: